

BECAUSE POSTPARTUM MATTERS
New Mom Gifts & Recovery Essentials, Delivered
Discover postpartum recovery must-haves, curated or custom gift boxes, and expert-written eBooks, all designed to support life after birth.

Featured Collections

































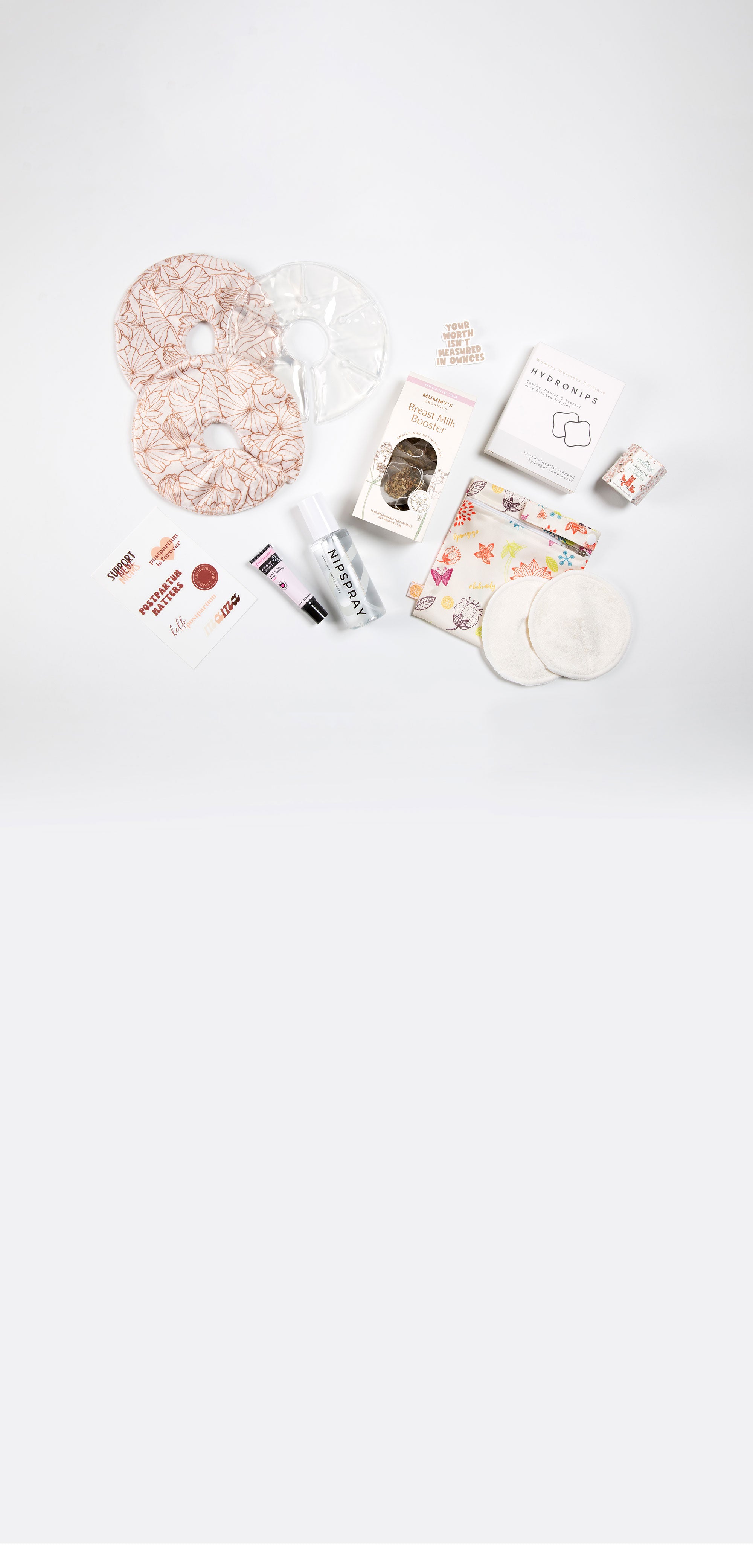
Build a Postpartum Gift Box
Select your items, we'll handle the rest.

AS SEEN IN






all-in-one support



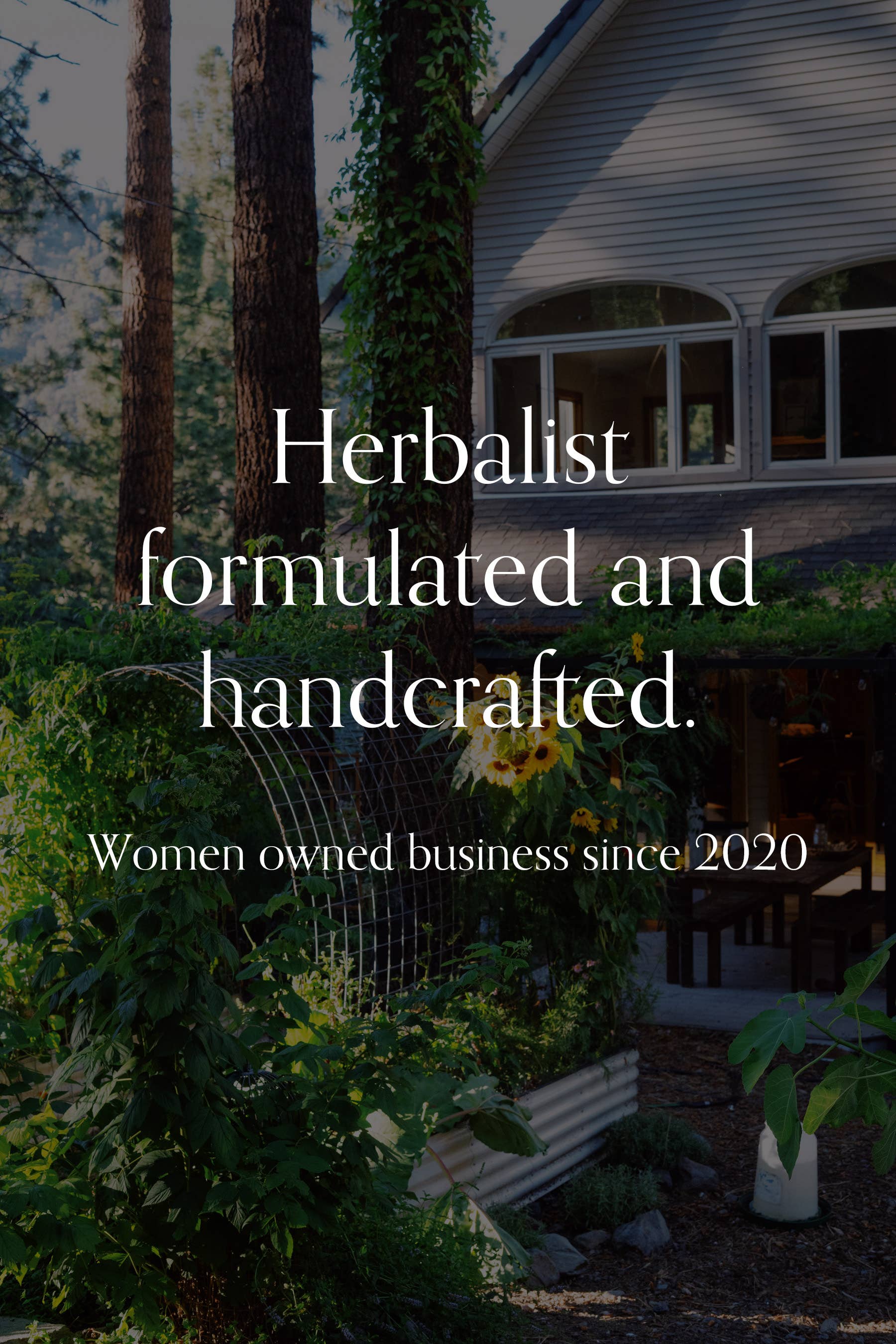
founded in 2020
About Hello Postpartum
We empower new moms through expert-created postpartum eBooks, recovery essentials, and supportive gifts. Baby doesn't need another swaddle, let's support life after birth for every new mom; one box at a time.























Carefully curated
About Our Products
Our products are high-quality, holistically-minded, safe for mom and baby, and from small businesses worldwide who are experts in postpartum care. Even better? 100% of our brands are women-owned (and the majority aren't available on Amazon).



Postpartum Journal






Let customers speak for us
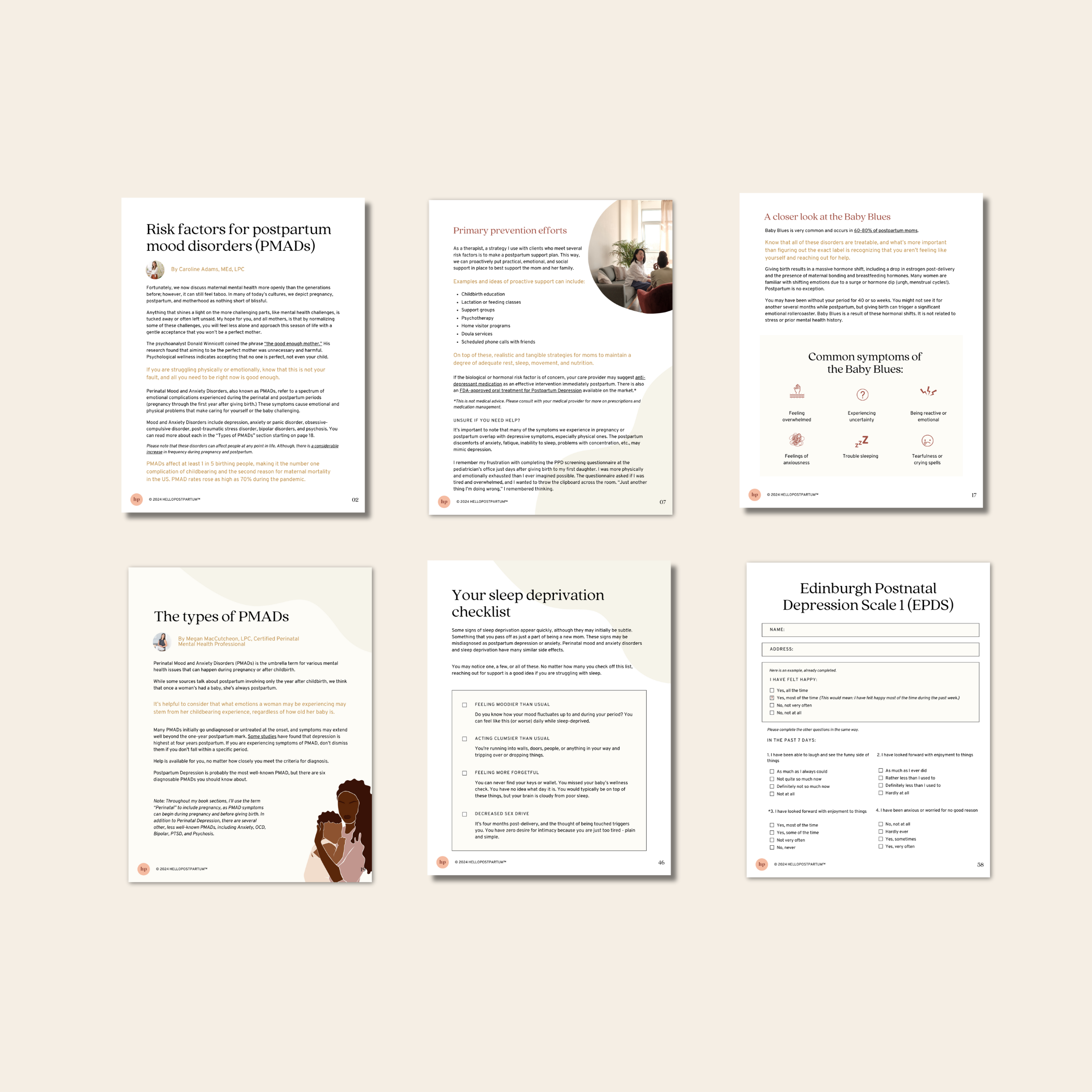
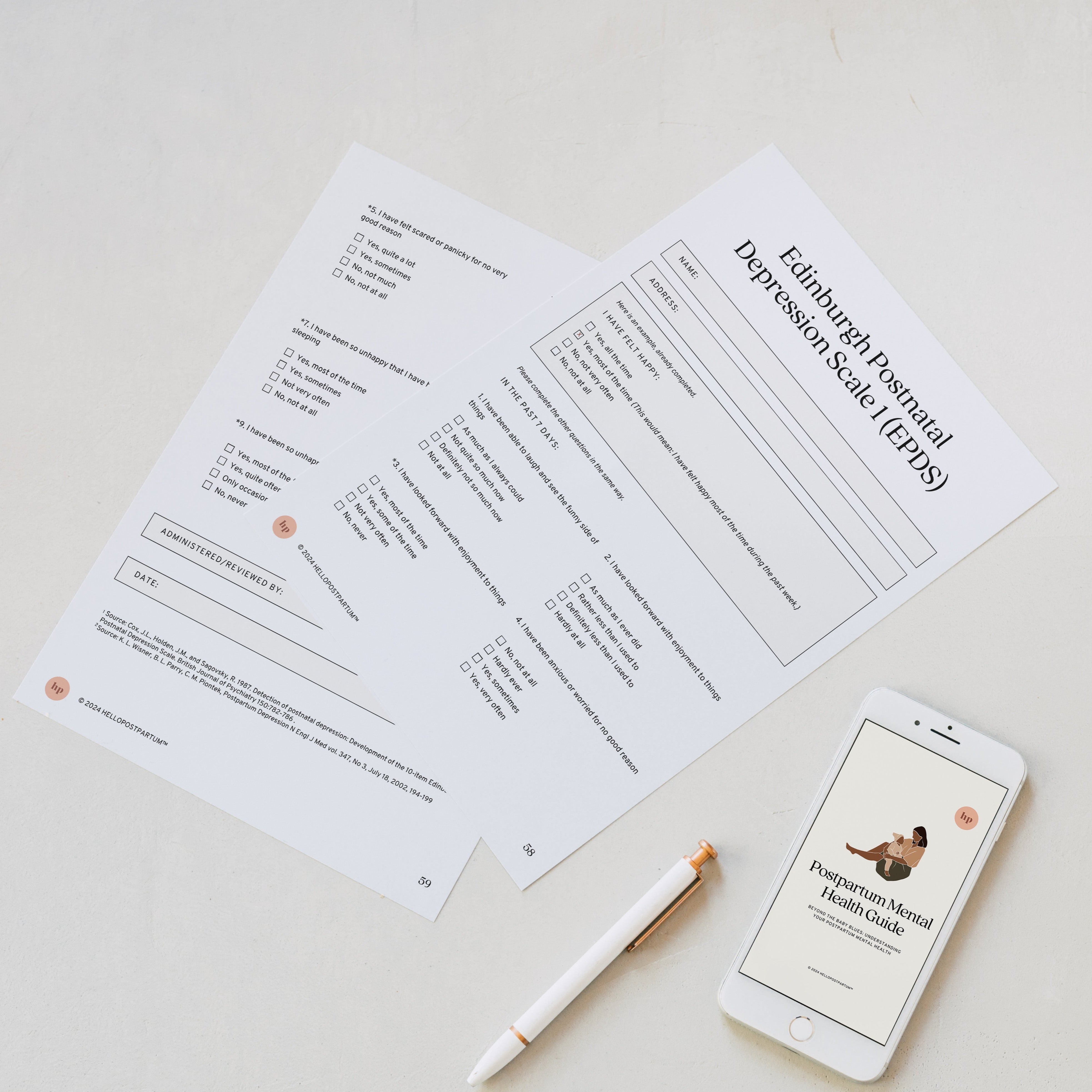
I’m really glad I stumbled upon this resource. My husband and I have friends that were really blindsided by unexpected postpartum mental health issues that resulted in the breakup of their marriage (they had issues to start with, though). They had no plan prior to both able how they would handle mental health issues as a team. We want to try our best to avoid that possibility, so we wanted to learn about what could happen and try to prevent it and then create a plan for what we agree ahead of time we should do if it does happen. We now know what the different issues are that can occur, how common they are, how to spot them, and how they differ from baby blues. We used this guide plus the free postpartum planning guide to know how to create a prevention plan. I printed out the checklist for us to just hang on the fridge so that we can see if I’m (or he is) meeting any of the criteria, and we are in the process of identifying a postpartum therapist that we can call on if needed in postpartum (plus we will try to see them once before birth to go over our plan with them and get their input). My husband and I have never had mental health issues before so I had no idea where to start in planning for preventing or coping with a postpartum mental health issue and after reading this I feel completely confident and prepared! As a health professional myself (Registered Dietitian) I also love that it was written by qualified health professionals and wouldn’t have purchased it otherwise!

Love that I could customize my gift basket to exactly what my girlfriend needed post partum 🫶🏼❤️ such a cool and special experience!

Cup came packed well so no damage occurred in transit

This high quality sticker allows for an open conversation about PPD without the pressure or stigma. It can easily be added to your water bottle as a beautiful reminder every time you see it that you are not alone.

Our dear friend, just had her baby three weeks ago and her pajamas arrived and she wore them for the first time two days ago. She absolutely loves them.!


Was delighted to get this top to use with my upcoming newborn. She isn't here yet, so I can't tell you how it works with a baby, but it's soft to the touch and easy to put on and figure out how to wrap. You can definitely wear it without a baby, while pregnant or with a newborn, so I don't feel like it's a top that is only for a short phase in life. I can definitely wear it as just a wrap top. Overall I definitely recommend!


Love this pouch, it is so soft and very cute design!

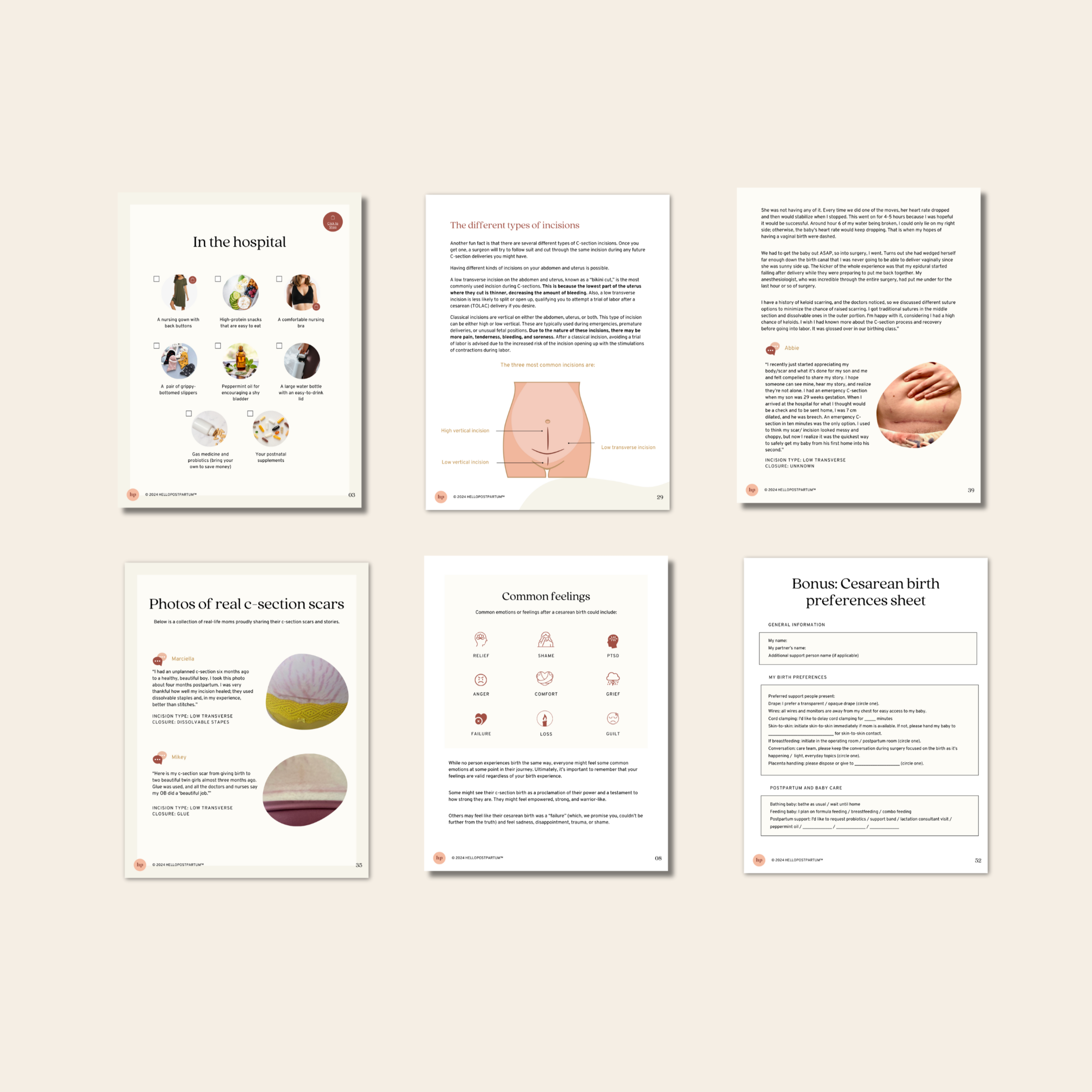
My friend had an emergency c-section and this was such a sweet personal gift to get to send her. She loved the items and I loved getting to pick each one out for her!
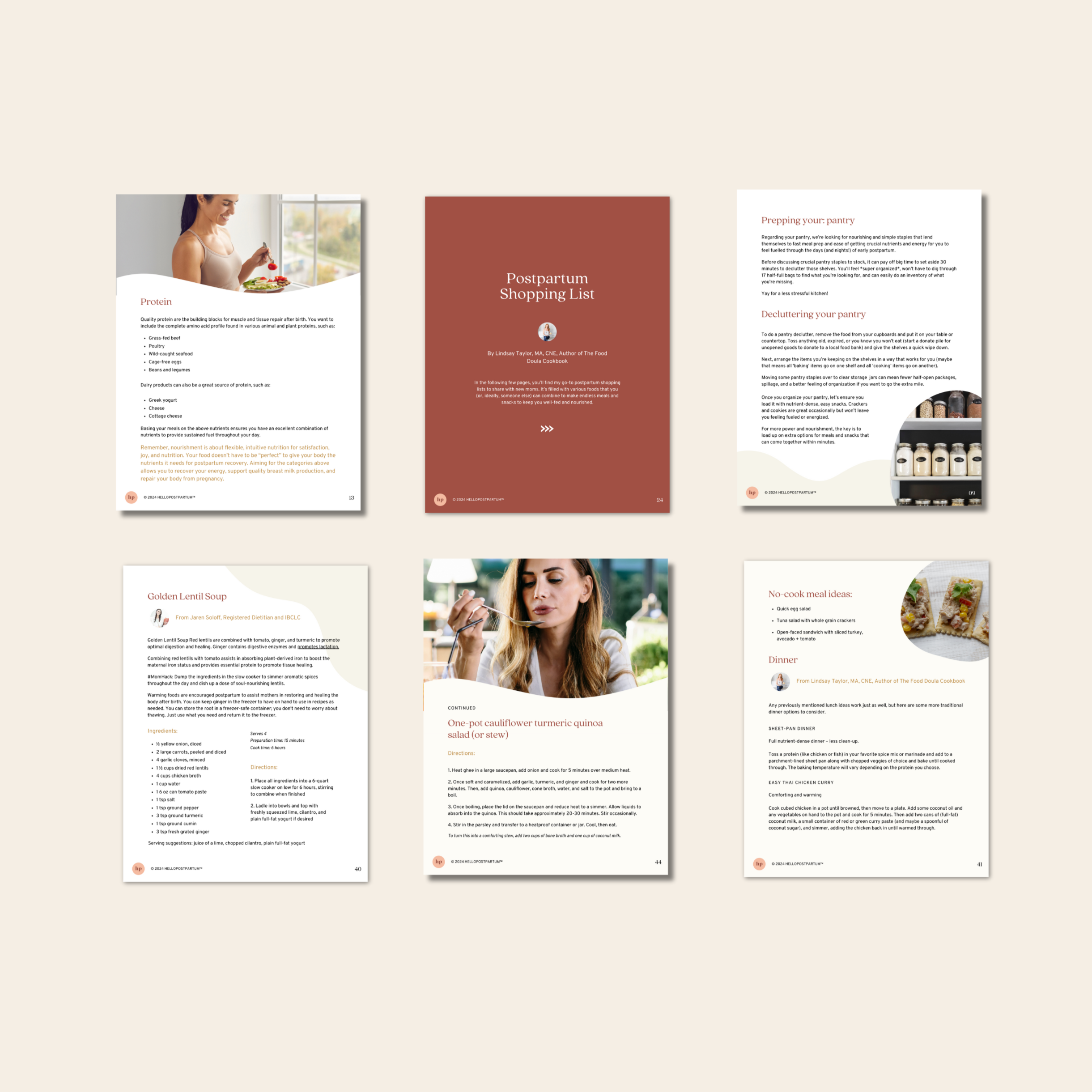
This book was absolutely perfect for what I was wanting and looking for! It’s laid out perfectly and makes postpartum food preparation so much easier! Thank you!

It was a pleasure ordering from here! I forgot to write a note on a card I had ordered and they promptly reached out and fixed it for me!

Everything in this box is great quality. We are picky about the type of consumables we use and it’s all well made and packaged.

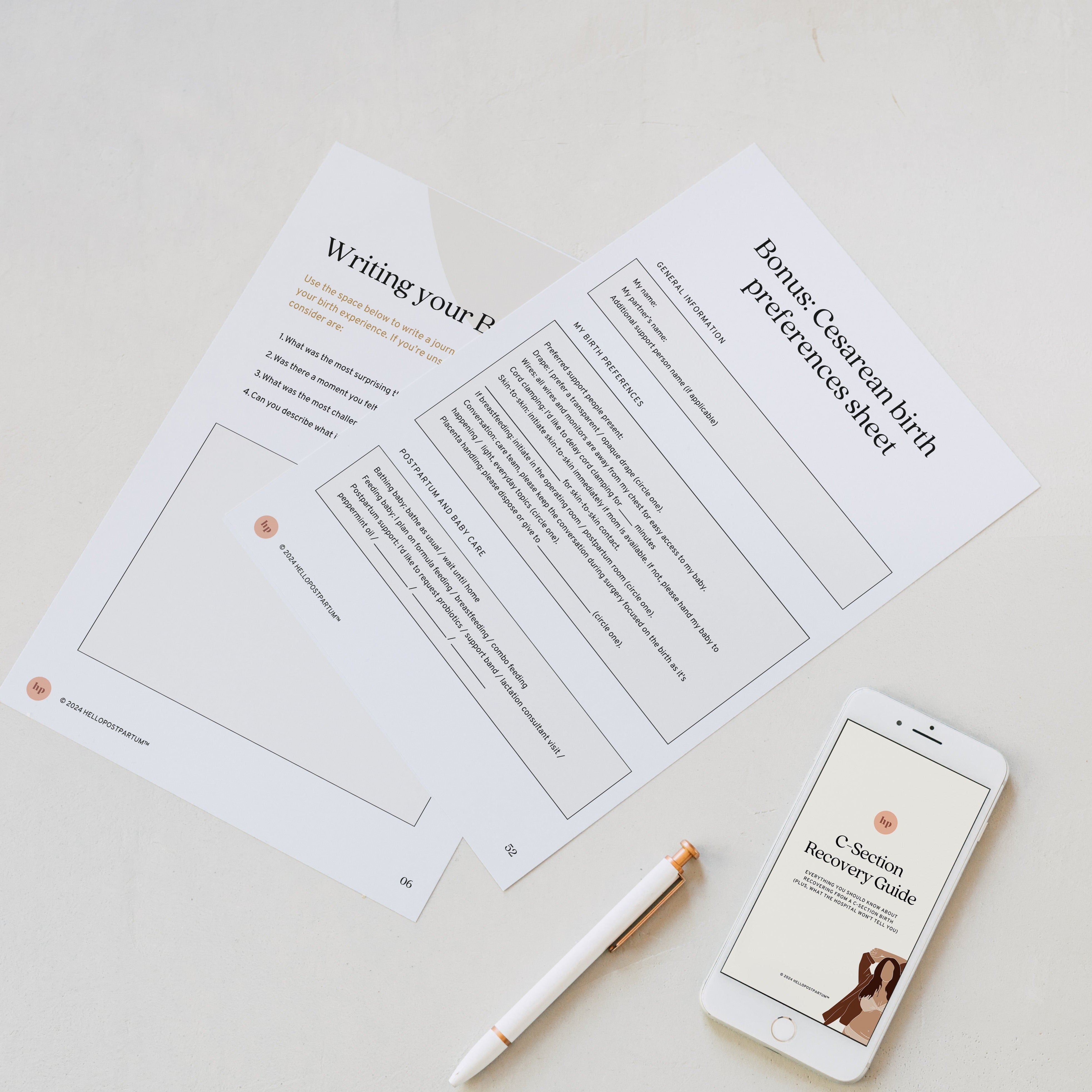
The e-book is very well done but I couldn’t download the c-section recovery guide. I don’t know why because with the others guide I didn’t have any problem.
Can you help me?
